You are here:
Home
|
What we do
|
Our Foundation
|
CSH Journal
|
Cutaneous genital schistosomiasis in …
Back to previous page
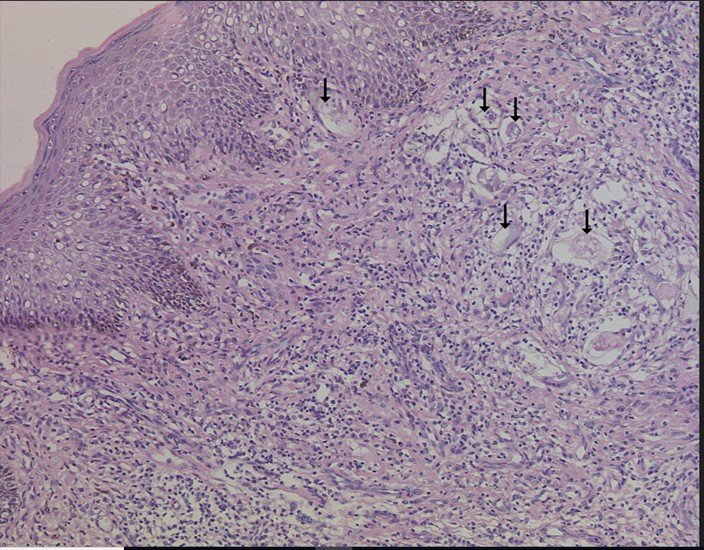
Cutaneous genital schistosomiasis in a 6-year-old female child - case report and review
1 Dec 2024
Case report
A six-year-old female child was referred to our dermatology clinic with a ‘growth’ involving her vulva that had been noted 8 weeks prior. Her mother stated it had gradually increased in size but had not bled and was not painful or pruritic. There were no additional symptoms such as fever, lower abdominal pain, dysuria, haematuria or vaginal discharge. She was from an area with freshwater bodies close to her home and as a child she often swam in them. Blood chemistries and blood count were within normal limits, no ova were detected in her urine or stool, and human immunodeficiency virus (HIV) status was negative.