Diagnostic clues of skin ulcers. Part I
1 Dec 2024
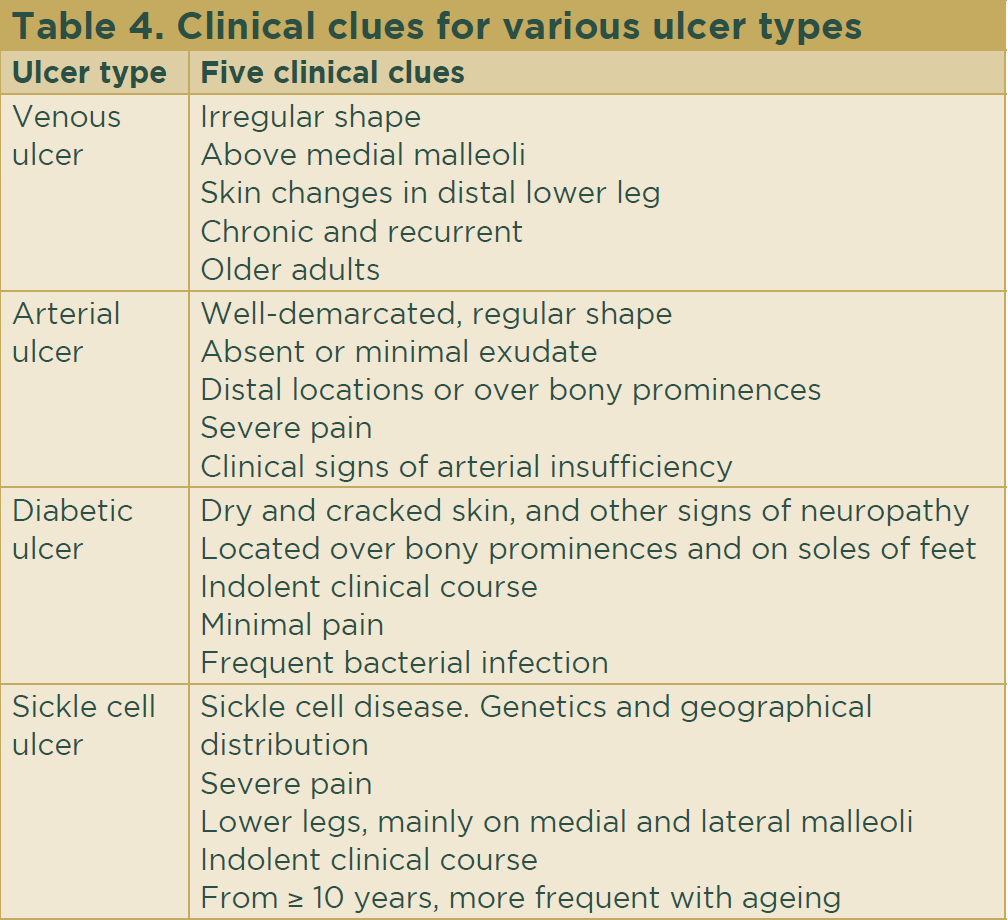
Venous ulcer
Venous leg ulcers, caused by venous insufficiency, are one of the most common lower limb ulcers. With a worldwide distribution, the estimated prevalence in the general population is 2%, rising to 5% among those > 65 years of age. These ulcers cause an important socioeconomic burden and a great psychological and physical impact on those affected.3 They are related to older age and are associated with a sedentary lifestyle and a genetic predisposition. Incompetence of the valves of the perforating veins connecting superficial and deep venous systems generates persistent high venous pressure. Clinical signs of venous insufficiency are purpura, hyperpigmentation, eczematization of surrounding skin, dermal fibrosis, an ‘inverted champagne bottle’ appearance of the leg and varicose veins. Venous ulcers follow an indolent clinical course, are frequently recurrent and are often related to external injury.

Venous and arterial insufficiency may coexist giving rise to a mixture of clinical features. Arterial ulcers cause severe pain that may worsen with limb elevation and in bed at night. Clinical suspicion is confirmed by determination of the ankle-brachial index and vascular imaging studies. Arterial ulcer treatment requires prevention and treatment of the underlying problems that compromise arterial flow (atherosclerosis, hypertension, hyperlipidaemia) and may also include referral for microvascular surgery.7