Diagnostic clues of skin ulcers. Part II: ulcers of infectious aetiology
1 Jul 2025
Introduction
Regardless of the causative agent, the clinical features of many infectious ulcers are very similar.
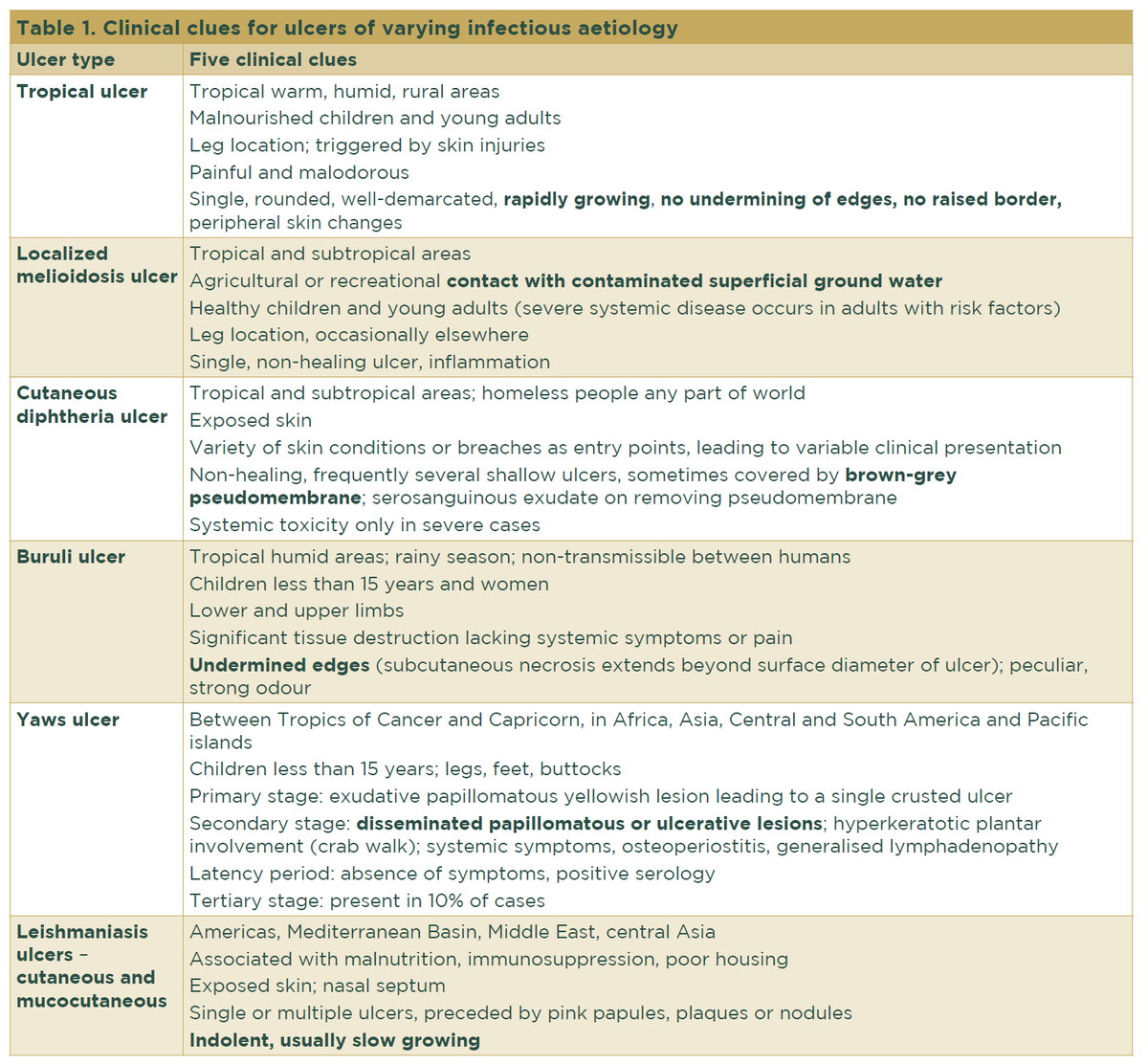
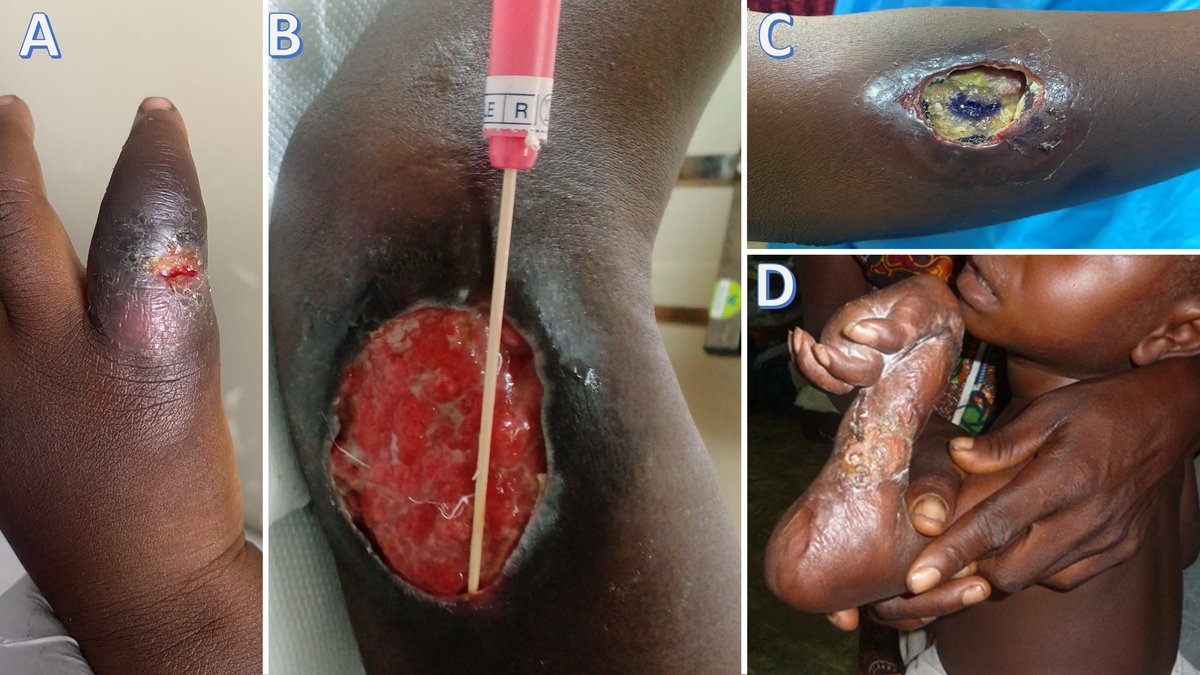
The most frequent infectious agents can vary between regions and over time. Some studies have found Haemophilus ducreyi (Figure 1a), Streptococcus pyogenes and other facultative anaerobic bacteria, Streptococcus dysgalactiae, Arcanobacterium haemolyticum, and Corynebacterium diphtheriae among the major causes of nonspecific skin ulcers 1,2

Buruli ulcer
Caused by the acid-fast bacillus Mycobacterium ulcerans, Buruli ulcer is the third most common mycobacterial infection after tuberculosis and leprosy. Cases are detected in the tropics in West Africa, the Americas, Asia, and the Western Pacific. Deforestation and anti-ecological practices favour Buruli ulcer development.6
M. ulcerans is isolated from soil, vegetation, standing or slow-flowing water, and various animals. Being non-transmissible between humans, mosquitoes and other insects are the suspected transmission agents. In southeastern Australia, Buruli ulcer cases are increasing, and the same M. ulcerans genome has been detected in infected individuals, mosquitoes, and possum faeces within geographical correlates.7
Treatment:
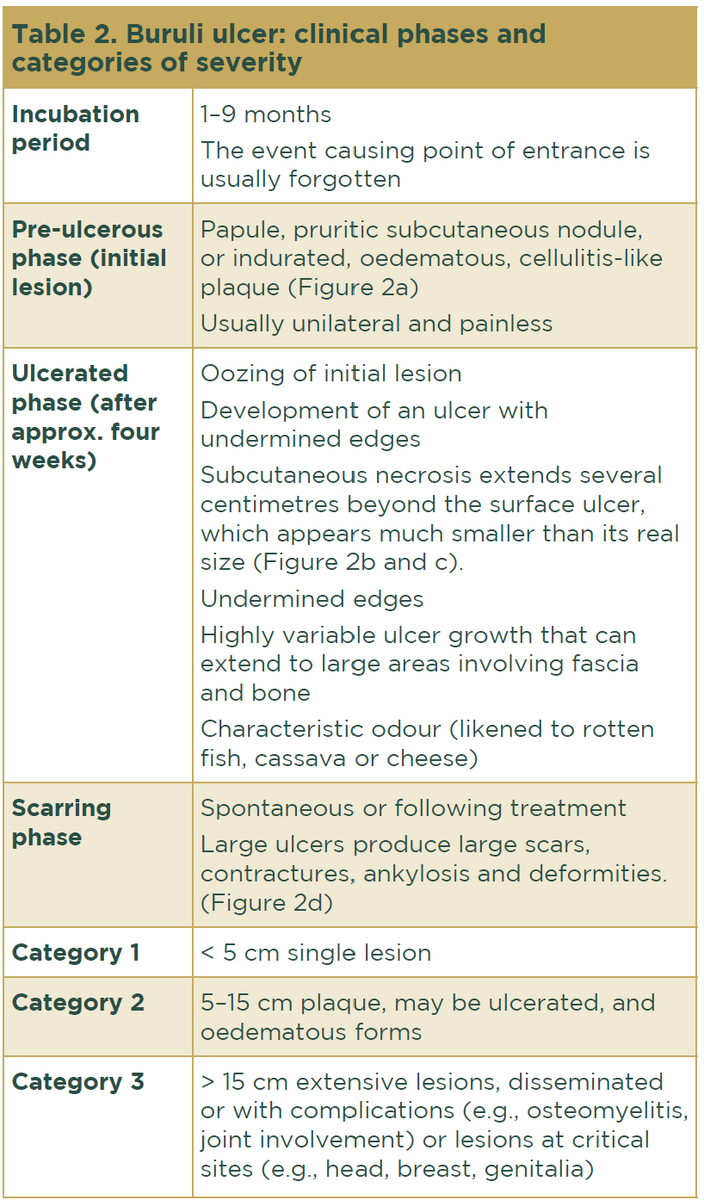
Buruli ulcer requires prompt recognition and treatment to prevent deformities and disabilities (Fig. 2D). Treatment includes different approaches.
Antibiotics
- First-line treatment: rifampicin 10 mg/kg daily for 8 weeks, plus clarithromycin 7.5 mg/kg twice daily for 8 weeks.
- Second-line treatment (recommended only for adults): rifampicin 10 mg/kg daily for 8 weeks plus moxifloxacin 400 mg daily for 8 weeks.
New shorter-duration regimens and new drugs effective against mycobacteria, e.g., telacebec, are under study.


Complicated cases are those with positive risk factors (Table 5). In this situation, systemic treatment is recommended. The options are as follows:
- Liposomal amphotericin B (high efficacy, but risk of nephrotoxicity);
- Systemic antimonial 20mg/kg/day IV or IM (very painful) for 10–30 days;
- Systemic antimonial plus pentoxifylline 400mg/8h for 10–20 days plus allopurinol 20mg/kg for 30 days in recurrent cases of L. tropica;