Epidemiological snapshot of dermatological conditions in a rural healthcare setting: a cross-sectional study in Belthangady, Dakshina Kannada District, Karnataka
1 Jul 2025
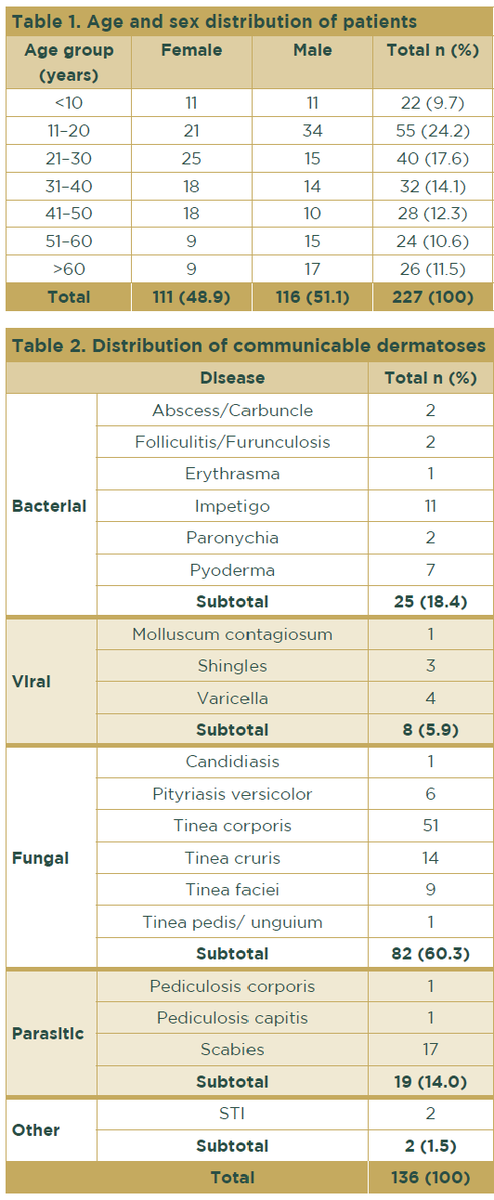


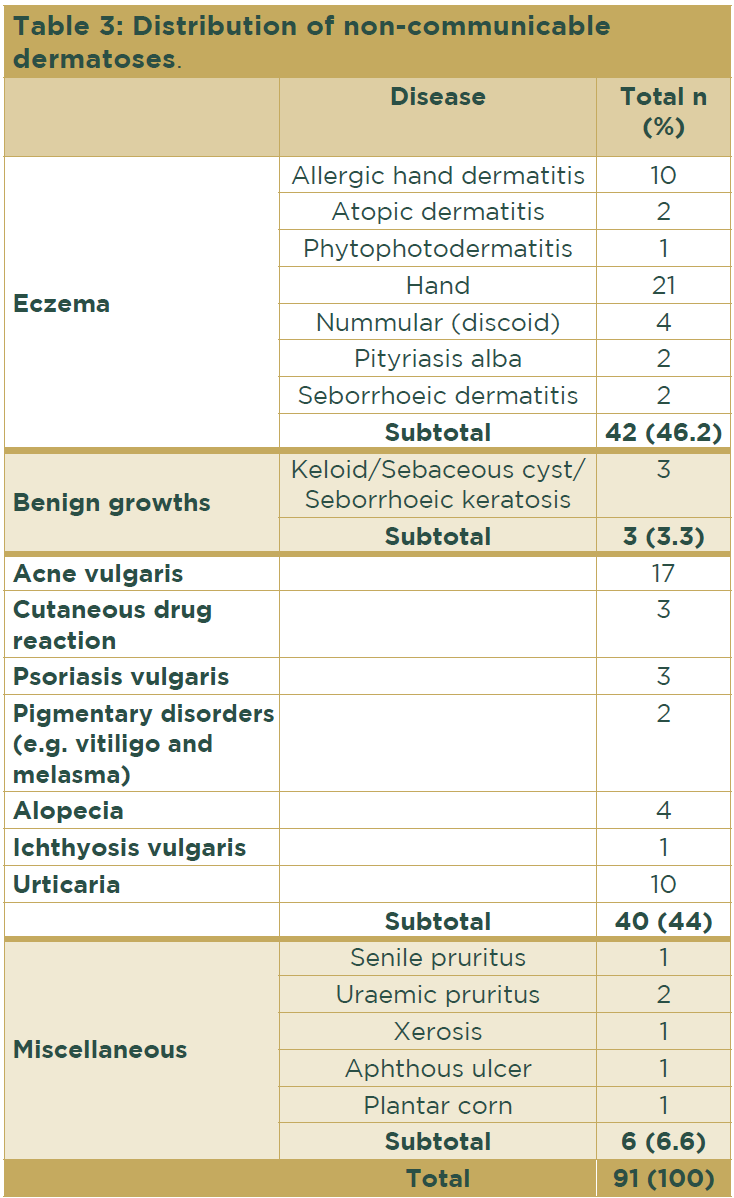
The prevalence of communicable disease (136 patients, 59.9%) surpassed that of non-communicable diseases (91 patients, 40.1%). Within the former group, fungal infections were the most prevalent, affecting 82 patients (60.3%), followed by bacterial infections, affecting 25 patients (18.4%) (Table 2). Among the fungal infections, the most frequent presentation was tinea corporis, identified in 51 individuals (62.2%). Scabies was the most common parasitic infestation, accounting for 17 patients (89.5%).

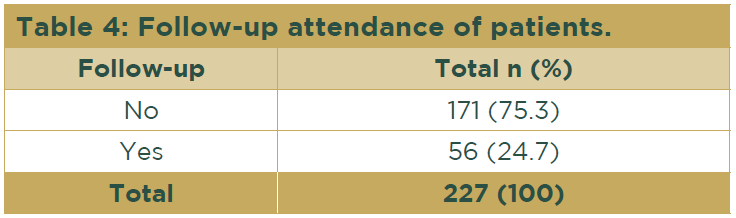
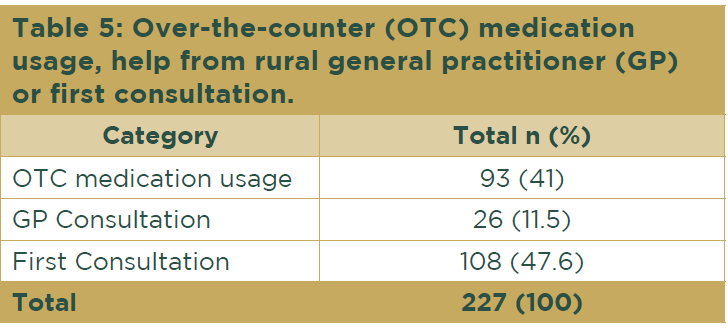
Overall, 93 individuals (41%) had used over-the-counter (OTC) medications obtained from pharmacies before seeking medical advice. In contrast, 26 patients (11.5%) had sought assistance from general practitioners, while 108 patients (47.6%) were attending their first consultation regarding their skin condition (Table 5).