Optimizing nutrition intervention to enhance wound healing in low-resource settings
1 Dec 2024
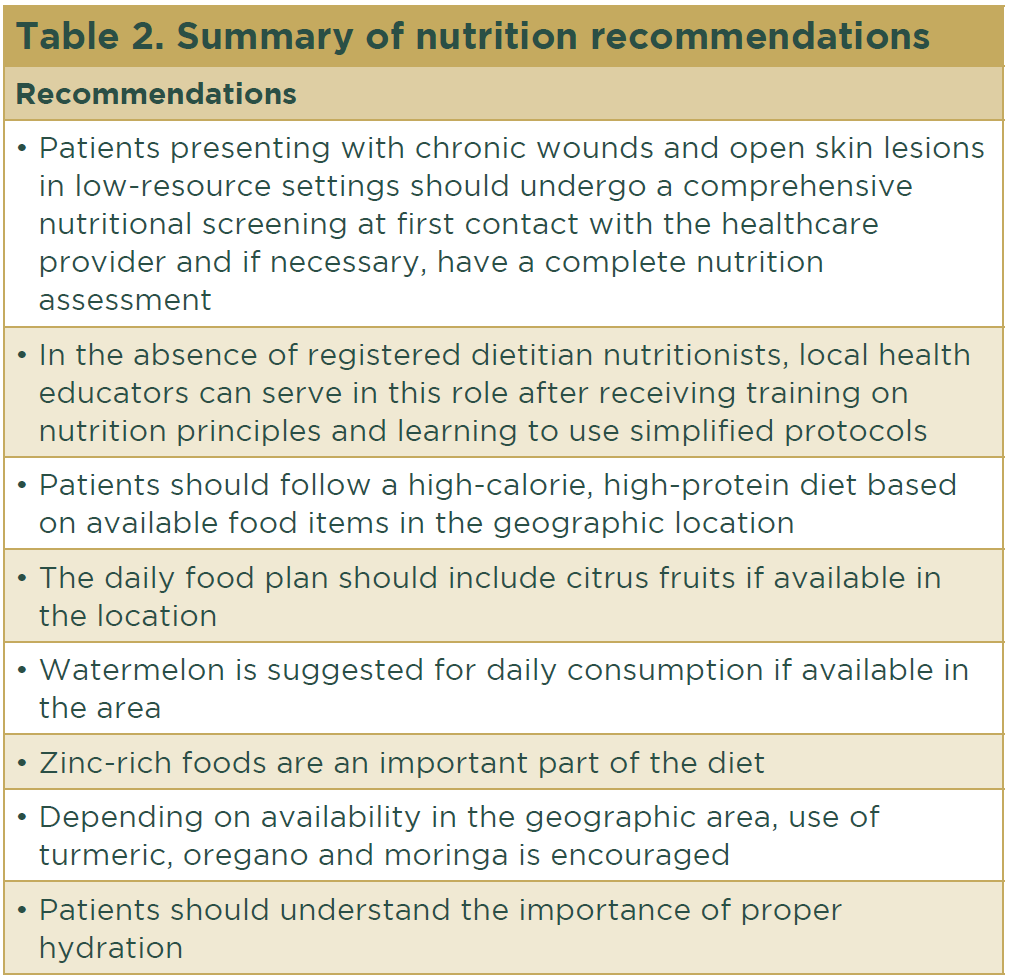
These phases and their biophysiological functions must occur in the proper sequence at a specific time and continue for a specific duration at an optimal intensity. Many factors can affect wound healing and interfere with one or more phases in this process, thus causing improper or impaired tissue repair.1 Table 1 summarizes the cellular and biophysiological events of each stage.
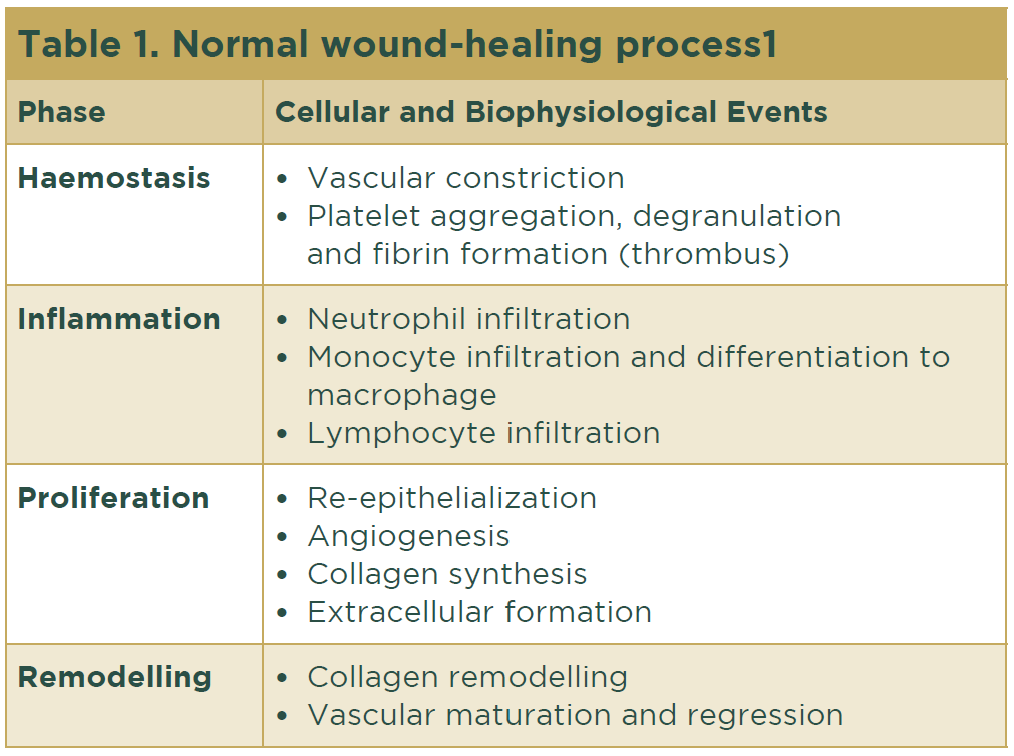
Vitamin C: Citrus fruits, including oranges, lemons, limes and tangerines, are abundant in many geographic areas, even those with low resources. The high vitamin C content of citrus fruits makes them ideal to provide vitamin C, which is a necessary daily cofactor for wound healing (Figs. 1 and 2).
L-citrulline and arginine: Food sources of citrulline are not abundant, with watermelon having the highest content of L-citrulline.9 L-citrulline is a precursor of arginine and currently is used extensively in commercial preparations of amino acid supplements because it provides higher levels of bioavailable arginine. Watermelon is an alternative where available.




Low-resource environments tend to lack adequate specialized staffing teams and hence are unlikely to have RDNs to manage and monitor nutritional interventions in patients with wounds. The use of trained local health educators is of immense value in patient nutrition education helping to improve wound-healing outcomes. No matter how low resource the setting is in terms of infrastructure and materials, concerned and compassionate human beings always can do something of value. The most precious resource available in these circumstances is other people.18